See how the Auryon System worked in real practice with diverse lesion types.
These case study outcomes are unique to the individual patient undergoing atherectomy procedures under the care of qualified healthcare professionals trained in the use of the Auryon System. Individual results may vary.
See how the Auryon System was used to ablate a total occlusion in the popliteal artery after unsuccessful attempts with crossing catheters.
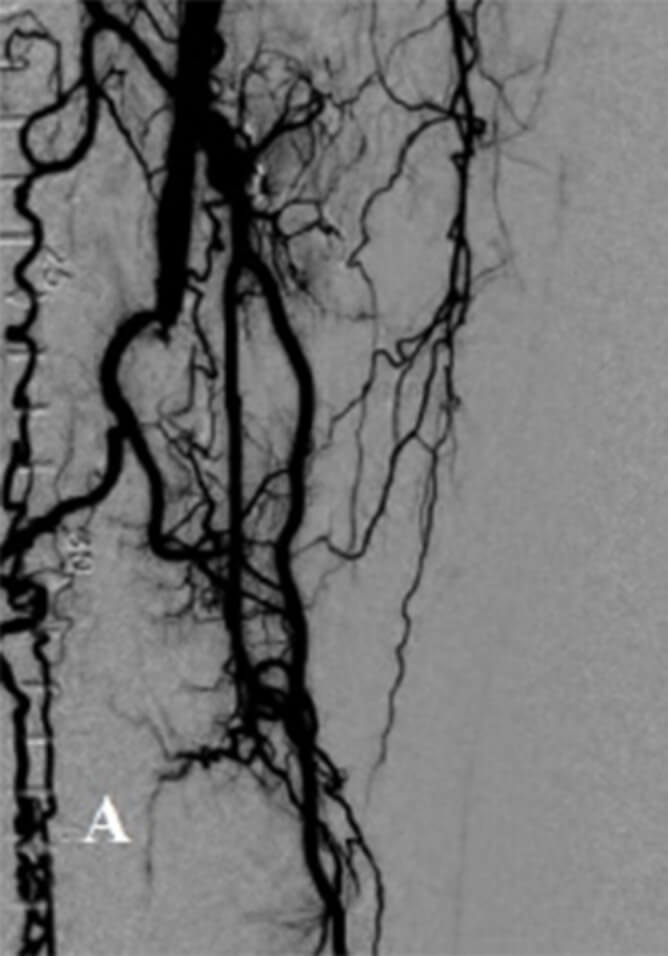
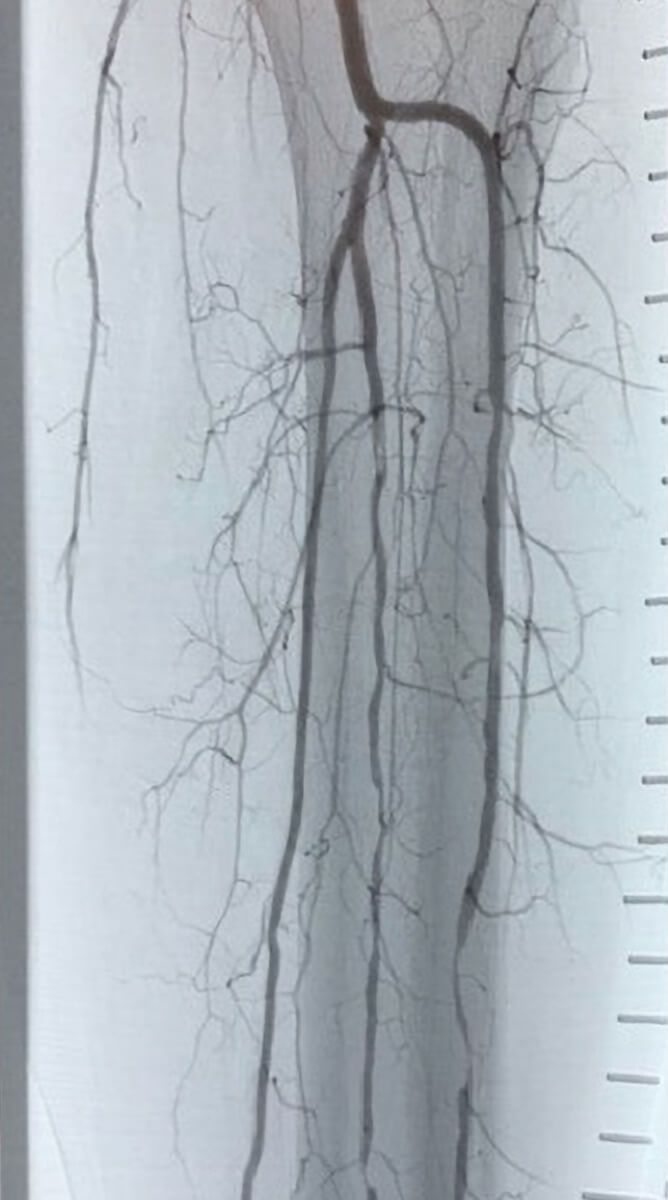
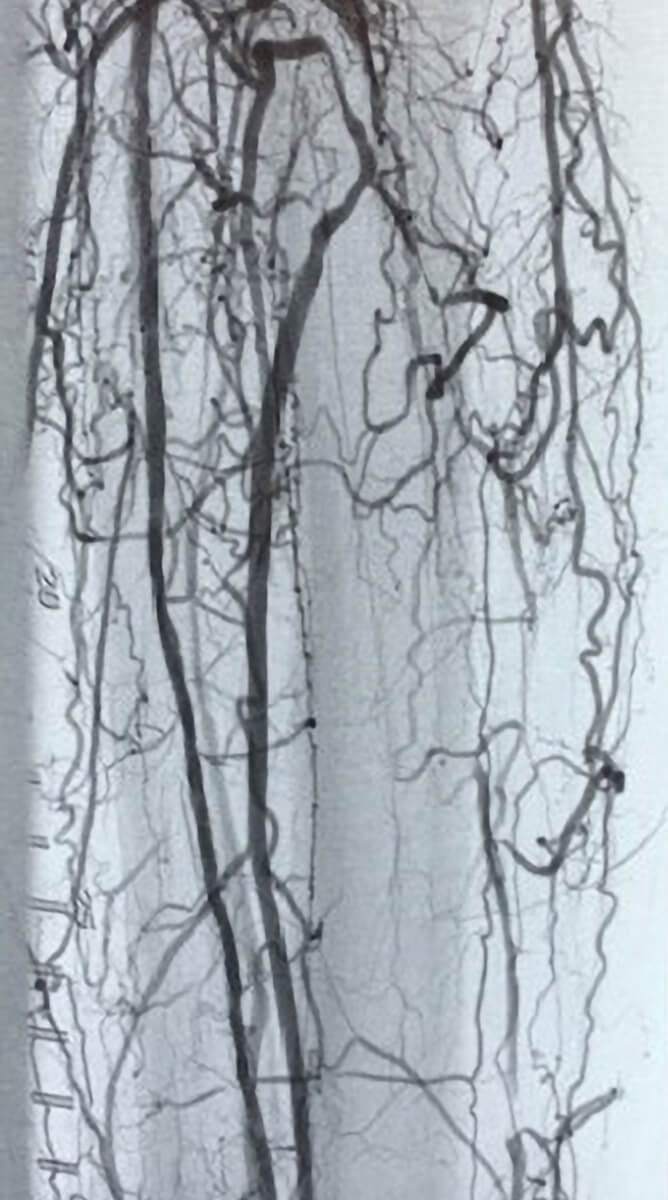
PRE AURYON LASER CTO IN THE SFA
PRE AURYON LASER CTO POPLITEAL

1.5mm AURYON LASER

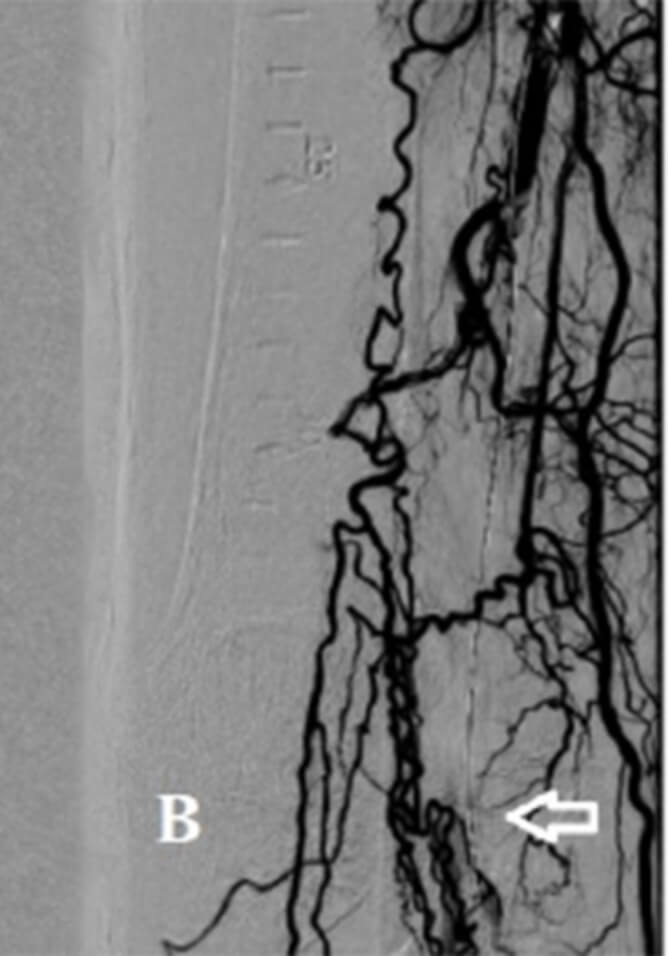
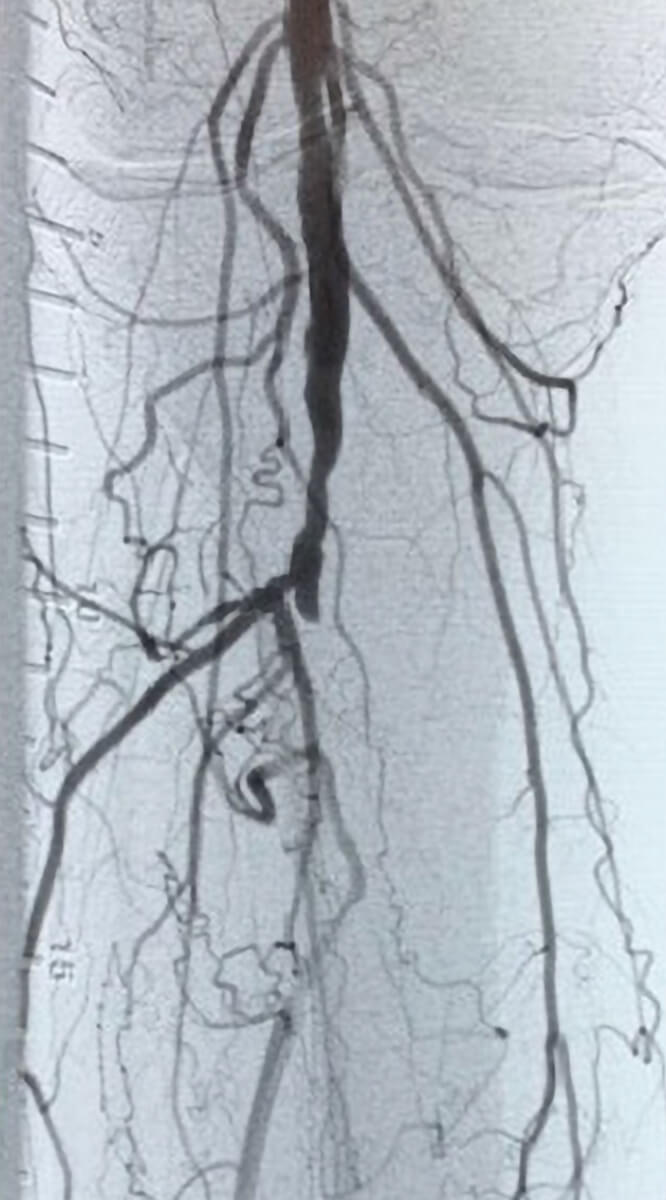
POST AURYON LASER PTA RESULTS POPLITEAL ARTERY
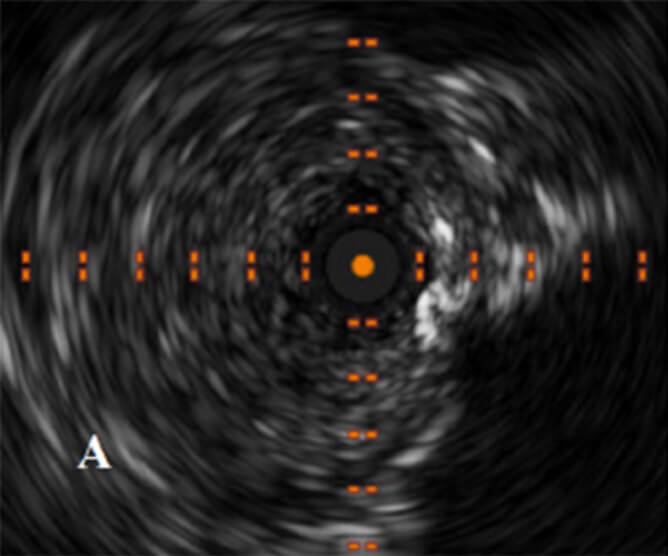
PRE AURYON LASER IVUS SHOWING CTO AND INTRALUMINAL POSITION OF WIRE
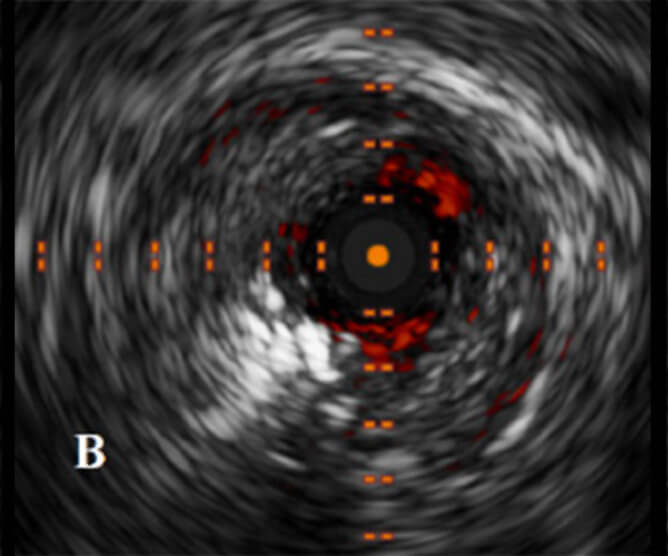
IVUS IMAGE POST AURYON LASER IN THE POPLITEAL ARTERY
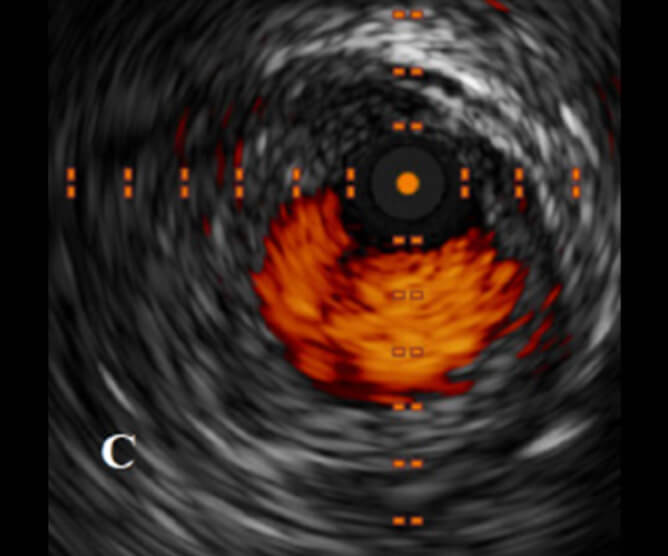
IVUS POST AURYON LASER AND PTA IN THE POPLITEAL ARTERY
See how the Auryon System was used to restore patency through atherectomy of the tibial and peroneal arteries.
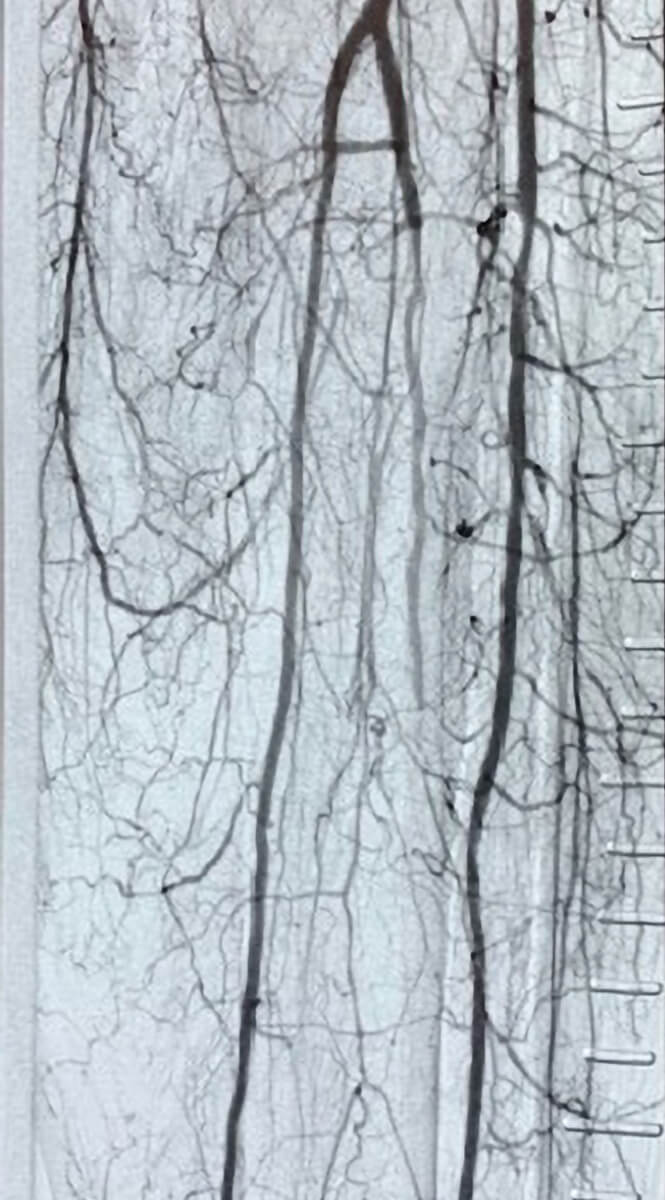
Pre-treatment with the Auryon System
Post-treatment with the Auryon System
See how the Auryon System was used to restore patency through atherectomy of the anterior tibial artery and the popliteal artery in 1 pass.
Pre-treatment with the Auryon System
Post-treatment with the Auryon System